Skip to content
About Us
News
Careers
Contact Us
About Us
News
Careers
Contact Us
Health
Individual / Family
Short-Term
Small Group
Dental
Vision
Life
Disability
Medicare
Medicare Advantage (Part C) | Know the Facts
Medicare Part D (Prescription Drug Plan)
Medicare Supplement Plans | What You Need to Know
Health
Individual / Family
Short-Term
Small Group
Dental
Vision
Life
Disability
Medicare
Medicare Advantage (Part C) | Know the Facts
Medicare Part D (Prescription Drug Plan)
Medicare Supplement Plans | What You Need to Know
Home
Health
Health Insurance
Short-Term Medical Insurance
Group Insurance
Dental Insurance
Vision Insurance
Life Insurance
Disability Insurance
Medicare
Medicare Advantage (Part C) | Know the Facts
Medicare Part D (Prescription Drug Plan)
Medicare Supplement Plans | What You Need to Know
About Us
News
Careers
Contact Us
Home
Health
Health Insurance
Short-Term Medical Insurance
Group Insurance
Dental Insurance
Vision Insurance
Life Insurance
Disability Insurance
Medicare
Medicare Advantage (Part C) | Know the Facts
Medicare Part D (Prescription Drug Plan)
Medicare Supplement Plans | What You Need to Know
About Us
News
Careers
Contact Us
Answer the Following Questions Accurately to Authorize Your Application!
Name
(Required)
First
Last
Phone
(Required)
Email
(Required)
Gender
(Required)
Male
Female
Are you on Medicaid or Medicare?
(Required)
YES
NO
Address
(Required)
Street Address
City
State
ZIP / Postal Code
County
(Required)
Primary Date Of Birth
(Required)
Month
Day
Year
Social Security Number
(Required)
Please Enter Your 9 Digit SSN NUMBER
Do You Have A Spouse To Enroll? *
(Required)
YES
NO
Full name Of Spouse
(Required)
Date of Birth
(Required)
Month
Day
Year
Social Security Number
(Required)
Name Of Employer
Terms and Condition
(Required)
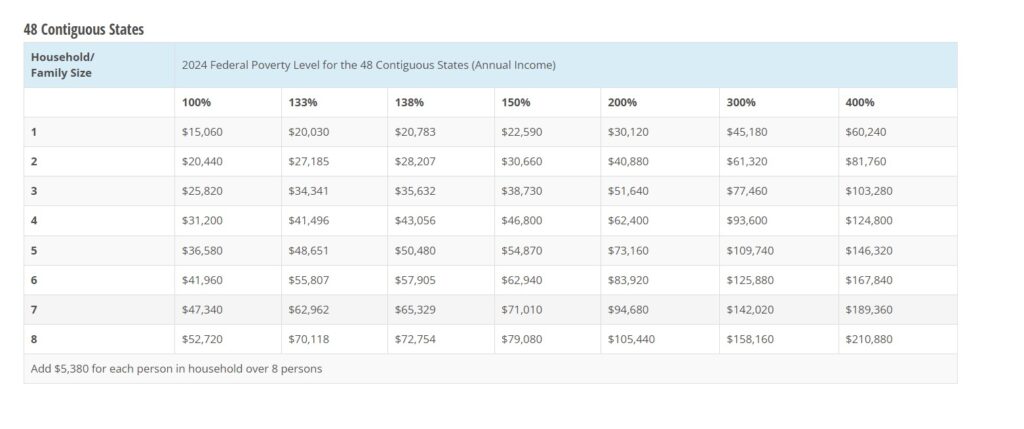
I give my permission to Alexander T Powell ISAOA/ATIMA to serve as the health insurance agent or broker for myself and my entire household, if applicable, for purposes of enrollment in a Qualified Health Plan offered on the Federally Facilitated Marketplace. By consenting to this agreement, I authorize the above-mentioned Agent to view and use the confidential information provided by me in writing, electronically, or by telephone only for the purposes of one or more of the following: Searching for an existing Marketplace application: Completing an application for eligibility and enrollment in a Marketplace Qualified Health Plan or other government insurance affordability programs, such as Medicaid and CHIP or advance tax credits to help pay for Marketplace premiums; Providing ongoing account maintenance and enrollment assistance, as necessary; or Responding to inquiries from the Marketplace regarding my Marketplace application for the next 60 months. I agree to be contacted by phone, email, SMS regarding my application. I understand that the Agent will not use or share my personally identifiable information (PII) for any purposes other than those listed above. The Agent will ensure that my PII is kept private and safe when collecting, storing, and using my PII for the stated purposes above. I confirm that the information I provided the Agent and the information used on my application is true and accurate. I understand that I do not have to share additional personal information about myself or my health with my Agent beyond what is required on the application for eligibility and enrollment purposes. I understand that my consent remains in effect until I revoke it, and I may revoke or modify my consent at any time by contacting my Agent at the following email address; info@futurewiseinsurance.com. Name of Primary Writing Agent: Alexander T Powell Phone Number: 2104693900 Email Address: info@futurewiseinsurance.com Agent NPN: 16776159 By submitting this document, you agree the above information is true and accurate. Also that your income falls in the following chart, qualifying you for the Zero Premium Health Coverage.
Terms and Condition
(Required)
I attest that my income qualifies for the tax credit.
Signature
(Required)
Δ